

CT
DENTASCAN
| The CT Dentascan is a specially developed computerized reformatting program that has been developed to obtain true cross-sections of the mandible (jaw) and maxilla (upper mouth) from the easily obtained CT scans for patients being considered for dental implant surgery in either the mandibular or maxillary arches. The main use of dentascans today is in the pre-operative planning and pre-operative modeling of endosseous dental implants and subperiosteal implants. When used appropriately, CT dentascans relieve a lot of the pre-operative guesswork by the patient's dental surgeon in the planning of the position and lengths of the implants when surgery is deemed possible and also assists in withholding surgery when it is not feasible. CT with the dentascan program eliminates the need to make strategic decisions after surgery has been initiated. It enables the dental surgeon to visualize the bony structures pre-operatively; the surgeon does not have to make decisions at the time of surgery when the mucoperiosteal flap is already elevated to visualize the bony structures directly. Dentascan CT provides the surgeons an operation with information of the internal structures that cannot even be gained by direct intra-operative visualization. |
|
 |
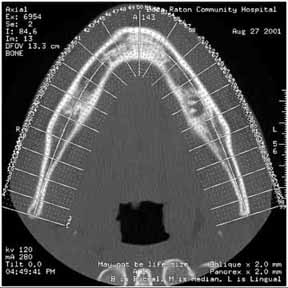 |
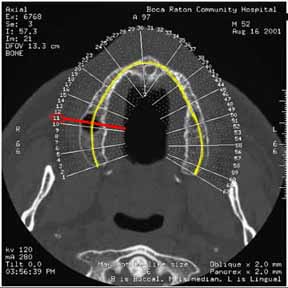
Figure 1 - Maxilla. Red line indicates slice #11 (see text). Yellow line indicates curvature of alveolar ridge |
Figure 2 - Mandible |
Axial scans at 1 mm are obtained continuously through either the maxilla (Figure 1) or mandible (Figure 2). Using the axial scan through the roots of the teeth, the curvature of the alveolar ridge is drawn on the computer screen (Fig. 1). Our software program then produces sequential oblique cross-sections every 2 or 3 mm around the entire curvature of the alveolar ridge. Each of the cross-sections is sequentially numbered and matched to tick marks on the axial views. Finally, five panoramic views are obtained and the oblique views are keyed to the panoramic scans as well.
The CT scans are photographed in true life-size format with vertical scale in millimeters.
 |
|
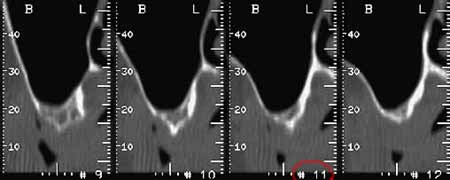
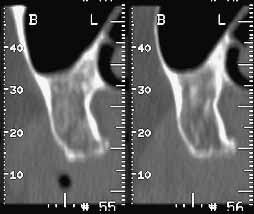
| Fig. 3 - Poor bone mass. Sequential sagittal reformatted images through maxilla (red circle indicates image #11 which corresponds to slice location in Figure 1). |
Fig. 4 - In a different patient, note the adequate bone mass in the maxilla compared to the patient in Figure 3. |
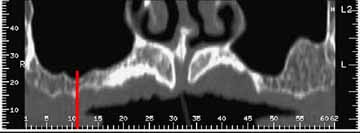 |
Fig. 5 - Maxilla- coronal panoramic reformatted view. Note vertical red line localizing slice #11 (see Figures 1 and 3) |
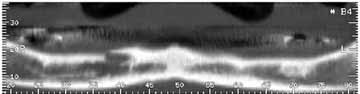 |
Fig. 6 - Panoramic reformatted view of adentulous mandible. Note poor bone mass throughout. |
|
The inferior alveolar nerve can be clearly seen on the cross-section oblique views (arrows). The inferior alveolar nerve canal is a vital structure that needs to be avoided during surgery. The anatomic features of the mandible most important to the
implant surgery are: |
 |
 link to Materialise website |
Surgery with regards to the maxilla is often a significant challenge without knowledge of the precise size and contours of the alveolar processes, frequently complicated by the paucity of the cortical bone to provide anchorage of the apical ends of the fixtures (Fig .3, 5) At Boca Raton Regional Hospital we also have the ability to send the CT dentascan computerized raw data on optical disc to the endoprosthesis manufacturers "Materialise" and "Columbia Scientific" who then are able to put the information on their proprietary software and submit their data in 3-D format to the dental surgeon who can plan surgery based upon direct measurements of his/her computer screen. |