

UTERINE ARTERY
EMBOLIZATION
(UAE)
aka
UTERINE FIBROID
EMBOLIZATION
(UFE)
aka
UTERINE FIBROID EMBOLIZATION (UFE)
BOCA RATON
REGIONAL HOSPITAL
DEPARTMENT OF
VASCULAR &
INTERVENTIONAL
RADIOLOGY
To schedule a consultation call: (561) 391-1728
REGIONAL HOSPITAL |
|
To schedule a consultation call: (561) 391-1728
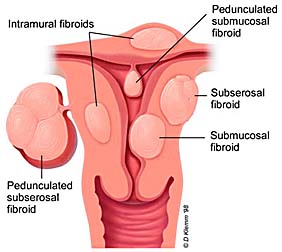
WHAT IS A UTERINE FIBROID?
- Benign tumor of uterine smooth muscle
- Fibroids are not considered to be pre-cancerous
- Also referred to as myomas or leiomyomas
- Types: submucosal, intramural, and subserosal
LOCATION OF UTERINE FIBROIDS
<link to source site>
HOW COMMON ARE UTERINE FIBROIDS?
HOW COMMON ARE UTERINE FIBROIDS?
- Estimated that 25 to 50% or greater of all women eventually develop fibroids
- Fibroids most frequent ages 30s & 40s
- Most common tumor of the pelvis in females
- A minority, perhaps 10% to 30% of these women are symptomatic
WHAT CAUSES FIBROIDS?
- Exact cause currently unknown
- Fibroids linked to estrogen
- Evidence that progesterone may stimulate fibroid growth
- ?Genetic Predisposition
WHAT SYMPTOMS OCCUR WITH UTERINE
FIBROIDS?
- Heavier menstrual bleeding, sometimes with passage of blood clots. Anemia can occur if bleeding is severe
- Pain, pressure, or feeling of fullness in the pelvis, abdomen, or lower back
- Frequent urination or constipation
- Pain during or bleeding after intercourse
- Infertility or miscarriage
HOW FIBROIDS ARE DIAGNOSED?
- Clinical history and Physical exam
- Pelvic Ultrasound (US) including Hysterosonography
- Magnetic Resonance Imaging (MRI)
- Laparoscopy or Hysteroscopy
HOW ARE FIBROIDS CURRENTLY TREATED?
- Small & No Symptoms -- follow with US and pelvic exam
- Mild Symptoms conservative, OTC medications, birth control pills
- Moderate Symptoms aggressive hormonal therapy (Lupron)
- Severe Symptoms--surgical, most commonly Hysterectomy or Myomectomy. Myolysis and Endometrial ablation less invasive options in select patients.
LUPRON
- GNRH agonist blocks ovarian estrogen production
- Advantages: Not Invasive, shrinks fibroids, often improves symptoms
- Disadvantages: Induces premature menopause and associated symptoms. Fibroids usually return to original size after cessation of therapy. Only used for short periods of time because of side effects
HYSTERECTOMY
- Surgical removal of uterus and fibroids, performed through abdominal incision or occasionally vaginally, sometimes with a laparoscope
- Advantages: 100% Curative, No risk of future cancer, Well established procedure
- Disadvantages: major surgery with potential surgical complications: infection, hemorrhage, injury to adjacent organs, adhesions, loss of child bearing potential, ?emotional, ?sexual
MYOMECTOMY
- Individual fibroids are resected through an abdominal incision or sometimes with a laparoscope or hysteroscope
- Advantages: Fertility can be preserved , well established procedure, less invasive if laparoscopic or hysteroscopic
- Disadvantages: Same potential surgical complications as hysterectomy; only part of uterus is treated and recurrence can occur; 15 to 25 % need repeat procedure, usually hysterectomy; not all fibroids amenable to myomectomy; adhesions can lead to infertility
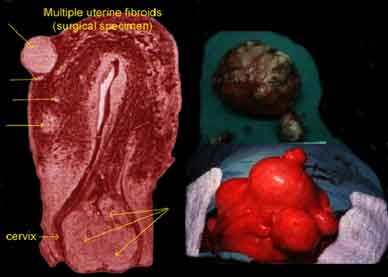
WHAT DO FIBROIDS ACTUALLY LOOK
LIKE?
HISTORY OF UTERINE ARTERY EMBOLIZATION
- Embolization of uterine arteries for severe post-partum or post-traumatic hemorrhage performed for nearly 20 yrs.
- Jacques Ravina, French Gynecologist 1990 Embolization prior to hysterectomy to decrease surgical blood loss
SERENDIPITOUS DISCOVERY
- Women noticed bleeding, pain, and bulk symptoms improved after Uterine Fibroid Embolization
- These women started to cancel their surgeries
- This discovery has lead to a promising new alternative treatment-UTERINE ARTERY EMBOLIZATION!
WHAT IS A VASCULAR AND INTERVENTIONAL
RADIOLOGIST?
- Highly trained Subspecialists skilled in both diagnostic imaging and technical catheter related procedures
- Vascular and Interventional Radiology has been referred to as "The Surgery of the 21st Century."


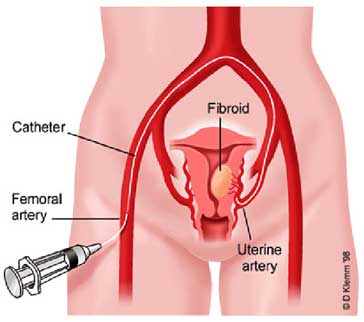
WHAT DOES THE EMBOLIZATION LOOK
LIKE?
| Schematic drawing of a catheter within the uterine artery and embolization of the arteries that supply the fibroids using Polyvinyl particles | 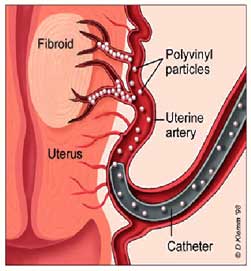 |
<link to source site>
HOW DOES UTERINE ATERY EMBOLIZATION WORK?
- Polyvinyl particles alcohol particles injected to block blood flow to fibroids
- Aimed at starving fibroids, by depriving them of blood supply
- Fibroids die (caseous necrosis) then scar down (hyaline sclerosis) and shrink
ANGIOGRAPHY SUITE aka
SPECIALS PROCEDURES
SPECIALS PROCEDURES

Using modern state of the art digital imaging equipment, the Interventional Radiologist works over the patient, in a sterile environment. This looks much like an operating room, except that high tech imaging equipment is used to help guide the doctor.
THE ACTUAL UAE PROCEDURE
- Angiography Suite, like an OR
with a modern million dollar X-ray machine, sterile conditions
- Epidural anesthesia and Conscious
Sedationby Board Cerified Anesthesiologist
- EKG, BP, HR, Resp., Oxygenation
monitored constantly during procedure
- Procedure typically takes one hour to complete
<link to source site>
PELVIC ARTERIOGRAM
This is an arteriogram of
the pelvic vessels during intial injection. One can see the enlarged
tortuous uterine arteries bilaterally.
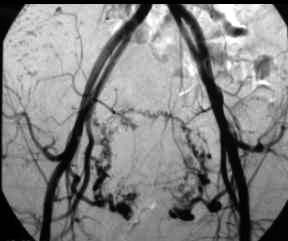
| This is an arteriogram of the pelvic vessels during intial injection. One can see the enlarged tortuous uterine arteries bilaterally. | |
PRE AND POST EMBOLIZATION
OF THE LEFT UTERINE ARTERY
OF THE LEFT UTERINE ARTERY

Injection of the left uterine
artery shows enlarged, tortuous arteries supplying the fibroids.
Cessation of blood flow forward
to the fibroids, with reflux of contrast to arteries in posterior
division of the left internal iliac artery following embolization.
| Injection of the left uterine artery shows enlarged, tortuous arteries supplying the fibroids. | Cessation of blood flow forward to the fibroids, with reflux of contrast to arteries in posterior division of the left internal iliac artery following embolization. |
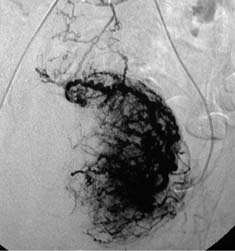
PRE AND POST EMBOLIZATION
OF THE RIGHT UTERINE ARTERY
OF THE RIGHT UTERINE ARTERY


Selective right uterine arteriogram
reveals enlarged, tortuous arteries supplying a prominent right
sided uterine fibroid.
Following successful embolization
of the right uterine artery there is no forward flow and back
filling of the proximal right uterine artery.
| Selective right uterine arteriogram reveals enlarged, tortuous arteries supplying a prominent right sided uterine fibroid. | Following successful embolization of the right uterine artery there is no forward flow and back filling of the proximal right uterine artery. |
PRE & POST EMBOLIZATION ANGIOGRAM
|
|
|
 |
 |
| Bilateral uterine artery injection again demonstrates enlarged tortuous vessels supplying the fibroids. | After successful embolization, there is no further flow of contrast, indicating no further forward flow of blood to the fibroids |
<link to source site>
WHAT TOOLS DO WE USE TO GUIDE
US INTO THE UTERINE ARTERIES?
US INTO THE UTERINE ARTERIES?




Angiographic Catheters
Guidewires
Microwires
|
|
|
|
|
|
|
|
|
WHAT IS POLYVINYL ALCOHOL?
WHAT IS POLYVINYL ALCOHOL?
| Polyvinyl particles (PVA), used to embollize the arteries that supply the fibroids are tiny synthetic "plastic" particles that are the size of fine grains of sand ranging from 0.3 mm to 0.7 mm in diameter. PVA has been used for more than 20 years in embolization of other parts of the body with no known reports of any adverse side effects due to this embolization material. |  |
POST-PROCEDURE CARE
- Overnight in hospital for pain management and observation
- Transient pelvic cramping 8-12 hrs after procedure relieved with epidural anesthesia. Nausea may occur and treated with antinausea medications.
- Discharge following morning with oral pain medication, NSAID's, and antinausea medications.
POST UAE AT HOME
- Mild to moderate cramping typically several days to a week
- Most women return to work in 3-4 days and report full recovery in 1-2 weeks
- 20% may develop temporary fever known as Post-Embolization Syndrome, can last up to one week. Treated with NSAID'S.
- Follow up appointment in 2 weeks. Follow up MRI in 3-6 months
UTERINE ARTERY EMBOLIZATION STATISTICS
- 85-90% of women have reported a partial improvement or complete resolution of symptoms, esp. decreased bleeding.
- 85-90% of women demonstrate on average 40-70% shrinkage in uterine and fibroid volume in 3-12 month follow-up
- > 90% of women reported satisfaction with the procedure
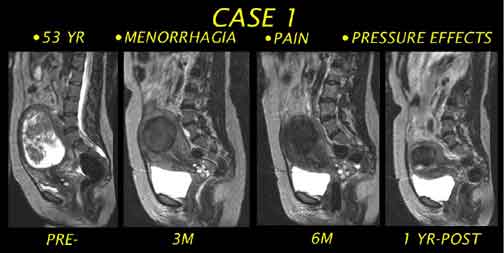
MRI OF THE PELVIS
PRE-EMBOLIZATION &
POST-EMBOLIZATION
PRE-EMBOLIZATION &
POST-EMBOLIZATION
<link to source site>
MRI OF THE UTERUS
PRE-EMBOLIZATION &
POST-EMBOLIZATION
PRE-EMBOLIZATION &
POST-EMBOLIZATION

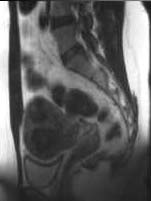
Pre-embolizaton MRI of the
pelvis reveals an enlarged fibroid uterus with maximum sagittal
length of 19.8 cm. Notice the anterior bowing of the abdominal
wall and mass effect on the bladder and sigmoid colon.
Six months post embolization
there has been interval reduction in size with the maximally
measuring 12.7 cm in sagittal length. Notice the decreased mass
effect on bladder and bowel with decreased bowing of the anterior
abdominal wall.
| Pre-embolizaton MRI of the pelvis reveals an enlarged fibroid uterus with maximum sagittal length of 19.8 cm. Notice the anterior bowing of the abdominal wall and mass effect on the bladder and sigmoid colon. | Six months post embolization there has been interval reduction in size with the maximally measuring 12.7 cm in sagittal length. Notice the decreased mass effect on bladder and bowel with decreased bowing of the anterior abdominal wall. |
MRI OF THE PELVIS PRE AND POST
EMBOLIZATION

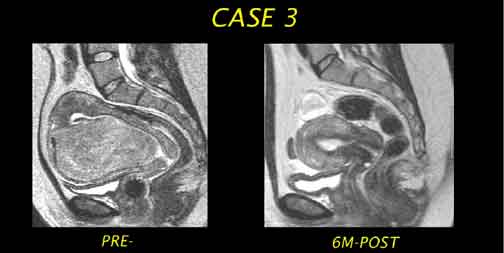
Sagittal image reveal an enlarged,
heterogenous fibroid uterus measuring 13.1cm in length.
3 months post embolization,
there has been moderate reduction in the size of the uterus,
measuring 9.9 cm in length with significant reduction in two
visualized dominant fibroids.
|
|
|
| Sagittal image reveal an enlarged, heterogenous fibroid uterus measuring 13.1cm in length. | 3 months post embolization, there has been moderate reduction in the size of the uterus, measuring 9.9 cm in length with significant reduction in two visualized dominant fibroids. |
MRI PELVIS PRE AND 6 MONTHS POST
EMBOLIZATION
(DRAMATIC RESPONSE)
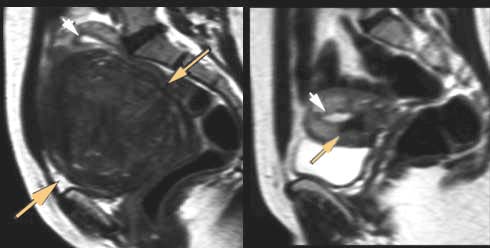
Prior to embolization, arrows
point to markedly enlarged 13 cm fibroid.
6 months post embolization,
there has been a dramatic response, the same fibroid now measures
2 cm
<link
to source site>
(DRAMATIC RESPONSE)
| Prior to embolization, arrows point to markedly enlarged 13 cm fibroid. | 6 months post embolization, there has been a dramatic response, the same fibroid now measures 2 cm |
<link to source site>
ADVANTAGES OF UTERINE ARTERY EMBOLIZATION
ADVANTAGES OF UTERINE ARTERY EMBOLIZATION
- Treats all fibroids simultaneously
- Minimally invasive, Complications infrequent
- No observed recurrence of treated fibroids in follow-up to nearly 10 years
- Shorter recovery period
- No adhesion (scar) formation
- Minimal blood loss. No need for transfusion
- Epidural and conscious sedation vs. general anesthesia
- Emotionally, physically, and sexually - UAE can have advantage over other treatments
DISADVANTAGES OF UTERINE ARTERY EMBOLIZATION
- 10-15% do not respond despite technical success
- Up to 2% of procedures technically unsuccessful
- Pelvic pain or cramping after procedure can remain moderate to severe for several days
- 1% to 2% chance of serious complication i.e. hysterectomy
- No tissue obtained for pathologic diagnosis
- Long term > 10 year follow-up not known
- Difficult to obtain. Operator experience often lacking
WHAT ARE THE RISKS OF UAE?
- Hysterectomy: 1% incidence due to uterine infection or infarction.
- Premature ovarian failure: 1% of patients experience amenorrhea. Most in late 40's.
- Radiation not considered dangerous
- Serious dye allergy is extremely rare
- Catheter related complications are rare in experienced hands
WILL UAE DECREASE FERTILITY?
- Conclusive studies with large numbers lacking
- Dozens of reported healthy pregnancies, with no reports of any adverse outcome due to UAE
- If infertility due to fibroids, fertility may improve in select patients after UAE. Research ongoing.
- Women with symptomatic fibroids desiring fertility probably should consider myomectomy first, especially if relatively uncomplicated.
WHO SHOULD NOT HAVE UAE?
- Women with asymptomatic fibroids
- Suspicion of malignancy
- Infection or pelvic inflammatory disease
- Pregnant women
- ? Peri-menopausal and Post-menopausal women
WHO IS A POTENTIAL CANDIDATE FOR UAE?
- Women with symptomatic fibroids: heavy bleeding, pelvic pain, bulk related symptoms
- Myomectomy or hysterectomy has been recommended
- Women who have a desire to preserve their uterus
- Women with aversion or desire to avoid surgery
- Women who have a desire to maintain fertility, if hysterectomy is only option
UTERINE ARTERY EMBOLIZATION
- Alternative to surgery for symptoms due to uterine fibroids.
- Studies, interviews and follow up exams based upon the several thousand UAE procedures make one thing quite clear:
Fibroid Embolization is a highly
successful,
minimally invasive alternative to hysterectomy
minimally invasive alternative to hysterectomy
MRI OF THE UTERUS
PRE-EMBOLIZATION &
POST-EMBOLIZATION
PRE-EMBOLIZATION &
POST-EMBOLIZATION
<link to source site>
UAE AT BOCA RATON REGIONAL HOSPITAL
- Initial Consultation: Call to obtain appointment. Bring all prior US, medical or surgical reports, and insurance information.
- Physical Exam and tests to rule out infection, Blood lab tests
- Pelvic MRI to document size and location of fibroids & rule out other diseases
CONTACT INFORMATION
Phone: (561) 391-1728
Fax: (561) 955-5015
Phone: (561) 391-1728
Fax: (561) 955-5015
[email us about UAE]
Website: http://bocaradiology.com
|
Boca Raton, Florida USA 33486
|
Free counters provided by Andale. |
Links to other Uterine Artery Embolization sites: |