

Vertebroplasty
(Non-Surgical Treatment of Compression
Fractures)
REGIONAL HOSPITAL |
 |
Background
Osteoporosis affects more than 30 million
Americans. Compression fractures occur in more than 500,000 patients
per year in the US, are more frequent than hip fractures, and
often result in prolonged disability. Risk factors include advanced
age, Caucasian or Asian race, low weight, diseases such as kidney
failure, and medication use such as prednisone. Current preventative
measures include calcium and vitamin D supplementation, exercise,
smoking cessation, and medications such as biphosphonates.
Management includes pain control with acetaminophen (Tylenol),
non-steroidals (Motrin), narcotics (Percocet), and bracing. Unfortunately,
the compression fractures often progress and develop at other
levels resulting in loss of height, disability, and secondary
complications from immobilization including pneumonia and pulmonary
embolism.
Percutaneous vertebroplasty has recently been introduced into the US as an effective therapeutic and preventative treatment for the pain and progressive loss of height in compression fractures.
What is Vertebroplasty?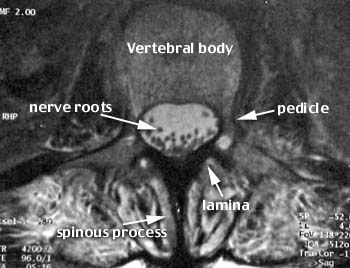
Vertebroplasty literally means fixing the vertebral body. A metal needle is passed into the vertebral body and a cement mixture containing polymethylmethacrylate (PMMA), barium powder, tobramycin, and a solvent are injected under imaging guidance by the physician. The cement hardens rapidly and buttresses the weakened bone. The barium makes the cement visible on x-ray and the tobramycin is an antibiotic. The procedure was originally developed in France in 1984 and has been further refined in the US since 1995.
How is Vertebroplasty performed?
Usually, the procedure is performed in an interventional radiology suite with special x-ray equipment (c-arm fluoroscopy) with nurses and technologists to help sedate the patient and operate the equipment. The patient is placed prone on the x-ray table and made as comfortable as possible. Sedation usually includes a narcotic (fentanyl) and a benzodiazopine (versed), which are short acting and can be reversed if necessary.
| The skin and underlying tissues are anesthetized with lidocaine and a special bone needle is passed slowly through the pedicle into the vertebral body using a slightly angled posterior approach. |  |
 |
| When the needle is in appropriate position, a small test injection with x-ray contrast is performed to ensure that a vein has not been entered. |
 |
| This prevents the inadvertent passage of cement into a vein and embolization to the heart and lungs. The needle is repositioned if necessary and the cement mixture is slowly injected during constant x-ray monitoring. When the potential spaces within the vertebral body are filled, the needle is slowly removed and the other half of the vertebral body is then filled with the cement. |
 |
It usually takes approximately 30-60 minutes to perform one level. More than one level can be performed if necessary during a single session. After the procedure, the patient is allowed to carefully ambulate and can usually go home within several hours. Most patients experience significant pain relief within the firsts 1-2 days. Many can stop their pain medications.
The Tools



Bone needles - Specifically made for smooth passage through bone, can also be
used for biopsy (Cook Medical Co.)

Tobramycin- an antibiotic powder used added to the cement to prevent infection
PMMA -polymethylmethacralate, A synthetic quick setting cement FDA approved for
human use in surgical procedures

Barium - an inert powder added to the PMMA cement to make it visible
on xray. It is manufactured by Bryan
Corp.
|
|
Bone needles - Specifically made for smooth passage through bone, can also be used for biopsy (Cook Medical Co.) |
Tobramycin- an antibiotic powder used added to the cement to prevent infection |
|
PMMA -polymethylmethacralate, A synthetic quick setting cement FDA approved for human use in surgical procedures |
Barium - an inert powder added to the PMMA cement to make it visible on xray. It is manufactured by Bryan Corp. |
Case Presentations
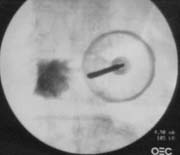
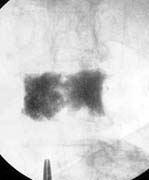
Case 1 - Osteoporosis
This patient suffered from painful compression fractures. One had already significantly collapsed while the other was just starting to collapse.
   |
 |
 |
These
images demonstrate injection of cement into both of these vertebral
bodies alleviating the pain and preventing further collapse. |
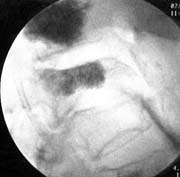
Case 2 - Metastatic breast cancer
| This patient had disseminated metastatic breast cancer to bone and had received both chemotherapy and radiation therapy. She developed paralysis and incapacitating pain. The MRI images show extensive bone tumor with collapse of the T10 and T11 vertebrae resulting in spinal cord compression. There was also extensive tumor in the T12, L2, and L4 vertebrae. Surgery with metal rod stablization was planned but there was fear that further vertebral body collapse would occur. Vertebroplasty was therefore performed at T12, L2, and L4. |  |
 |
 |
 |
The patient's paralysis quickly resolved with steroid administration (decreased tumor swelling) and her pain was markedly decreased following the vertebroplasty. She left the hospital without having any surgery.
Risks of Procedure
1) Leakage of cement into veins and or lungs
2) Infection
3) Bleeding
4) Rib or Pedicle fracture
5) Pneumothorax
6) Worsened pain
7) Paralysis secondary to leakage of cement
It should be noted that there have been very few reports of serious complications form this procedure in the US.
What are indications for Vertebroplasty?
1) Painful compression fracture secondary to osteoporosis
2) Painful compression fracture secondary to tumor which does not respond to conventional therapy
3) Prevent further compression fractures
4) Buttress weakened bone for spine fusionsPlease note that the procedure is generally used for the first indication and is rarely used for the others.
Relative Contraindications
1) Young patient - the long term effects of the cement mixture are unknown
2) Vertebral bodies above the T5 level - the procedure is riskier and more difficult
3) Patients with prior unsuccessful spine surgery
Patient Evaluation
1) History and Physical Examination
2) Current x-rays
3) MRI +/- bone scan
Follow Up Care
1) Pain medications - usually tapered over several days after procedure
2) Muscle relaxants
3) Adjust medications to prevent further mineral loss
Vertebroplasty Statistics
1) >80% moderate to marked pain relief
2) <5% induced fractures from procedure
3) <1% symptomatic embolism or infection
Contact Information
Director, MRI and Neuroradiology Boca Raton Regional Hospital Boca Raton, Florida USA |
 |
Phone: (561) 391-1728 Fax: (561)
955-5015
E-mail: JWiener@BocaRadiology.com
Website: http://BocaRadiology.com
|
Boca Raton, Florida USA 33486 |
 American Society of Neuroradiology, a subspecialty organization committed to excellence in clinical care and research in imaging and therapy of neurological disease |
|
