

Breast MRI Cases
Boca
Radiology Group is pleased to offer state of the art services in breast
MRI. We
use a dedicated high signal to noise breast coil on our 1.5 Tesla magnets.
Our protocol combines high bilateral spatial resolution (3D gradient
echo with 512 matrix and 2mm slices of both breasts) with multiple
acquisition time points to evaluate the kinetics of tissue enhancement
following dynamic bolus gadolinium administration. Pathologic tissues
can be identified by their morphology (shape and solid/cystic nature)
as well as by their vascularity and permeability (kinetics). Special
post processing software provided by our partner in breast MRI research, Mevis
Technologies has been moved to a more user friendly Windows
2000 Professional interface (DynaCAD™) from
the Silicon
Graphics platform. This allows rapid evaluation of large breast
MRI data sets in 1- 2 minutes with full 4-Dimensional display (3 orthogonal
spatial plus time dimensions with color encoding of enhancement curves) as
well as automated 3D motion correction (DYNA Motion) and 3D MIP color
overlay (Dyna MIP).
We
have conducted a prospective clinical trial of breast MRI's
ability to stage breast cancer in collaboration with the Weizmann
Institute in Israel and Mevis in Bremen, Germany. We have
found that MRI of the breast allows more accurate staging of the extent
of breast cancer than mammography and ultrasound. Our post-processing
techniques yield higher sensitivity and specificity than interpretation
of the raw image data alone. Patient management is significantly changed
in many cases. For example, detection of more extensive disease
in the breast of concern often leads to mastectomy rather than lumpectomy
and cancerous lesions in the opposite breast are often discovered.
We
are also evaluating newer software applications including 3D motion
correction (DYNA Motion), 3D MIP color overlay (Dyna MIP) with our
partner Mevis Technologies.
<click
here to download a 3 minute video (24MB, wmv format) demonstrating
MRI-guided breast biopsy>
Clinical
cases:
Case
1
This
61 year old female presented with a dominant mass in the right breast
with several other indeterminate lesions seen on mammography.
Mammography
CC view  demonstrates
three masses in the right breast, one behind the nipple and two others
in its medial portion.
demonstrates
three masses in the right breast, one behind the nipple and two others
in its medial portion.
MRI
magnification maximum intensity projection (MIP) view of
right breast demonstrates the same three masses with tumor bridging
between them and extending toward the chest wall.
of
right breast demonstrates the same three masses with tumor bridging
between them and extending toward the chest wall.
MRI
T2 axial slice indicates
cystic nature of subareolar mass.
indicates
cystic nature of subareolar mass.
MRI
subtraction and color
images show
rim enhancement around cystic mass.
and color
images show
rim enhancement around cystic mass.
MRI image of color
map of enhancement curves (kinetics
of breast tissue) show intense early enhancement and rapid signal
loss from the dominant mass (typical malignant characteristics).
Enhancement
curve from dominant mass .
.
Final Pathology
at mastectomy confirmed that the dominant mass represented infiltrating
carcinoma with extension of intraductal carcinoma. The subareolar
cystic mass represented encysted papillary carcinoma.
Case
2
This second 61
year old female presented with micorcalcifications on mammography.
Mammography
CC view demonstrates
a circled suspicious area of microcalcifications in the left breast
which are better demonstrated on the magnification
view
demonstrates
a circled suspicious area of microcalcifications in the left breast
which are better demonstrated on the magnification
view .
.
Post-processed
color parametric map image demonstrates
a large area of malignant enhancement in the central left breast.
demonstrates
a large area of malignant enhancement in the central left breast.
These findings
indicated a much more extensive area of malignancy to the breast surgeon
which allowed accurate pre-operative needle localization and subsequent
segmental resection with negative margins. Image guided biopsy and
surgical pathology specimen revealed extensive intraductal carcinoma
(comedo, solid, and cribiform types) with extensive cancerization of
lobules. Two small foci of well differentiated infiltrating ductal
carcinoma were also identified.
Case
3
This patient
underwent mastectomy, radiation therapy, and subsequent breast reconstruction.
On a follow up clinical examination, there was palpable thickening
raising the question of recurrent cancer. An MRI excluded recurrence. The maximum
intensity projection image
demonstrates enhancing vessels while the color
map image
image
demonstrates enhancing vessels while the color
map image demonstrates
normal arterial vascularity at the margins of the reconstruction.
demonstrates
normal arterial vascularity at the margins of the reconstruction.
Case
4
An example of
an obvious cancer
in the right breast with
motion artifact resulting in a false eccentric malignant rim of enhancement.
with
motion artifact resulting in a false eccentric malignant rim of enhancement.
The movie demonstrates
a comparison of the original post-processed data set (left hand
images) using a rainbow color map with the most malignant enhancement
demonstrated in red. The motion corrected data set is on the
right. Note that the artifactual background areas of color have
largely disappeared and that the tumor now shows symmetrical peripheral
malignant enhancement.
demonstrates
a comparison of the original post-processed data set (left hand
images) using a rainbow color map with the most malignant enhancement
demonstrated in red. The motion corrected data set is on the
right. Note that the artifactual background areas of color have
largely disappeared and that the tumor now shows symmetrical peripheral
malignant enhancement.
Case 5
58 year old woman with indeterminant calcifications central right
breast. Fatty
Enbloc procedure: DCIS


MRI: biopsy cavity with 2cm enhancement posteriorly suspicious for
invasive disease
Surgery: IDC, negative sentinel nodes
Points
MRI can better predict the extent of disease than mammography even
in the fatty breast
Surgical management may change as a result of pre-operative MRI: sentinel
node was performed preventing second surgery, wide localization performed
appropriately to avoid positive margins
Case 6
The patient is a 69 year old woman presenting with a 2 cm left axillary
mass found to be adenoCA compatible with breast primary. Negative prior
mammogram
MRI identified 2 small suspicious masses in the UOQ


Diagnostic mammogram & US demonstrated 2 spiculated solid masses
which corresponded
US core biopsy found 2 IDLC
Lumpectomy and axillary dissection was performed
Points
MRI is valuable in the evaluation of a patient with axillary disease
with unknown breast primary
Targeted mammography and US performed after MRI will often identify
abnormalities which then can be biopsied with US or stereotactic guidance
Case 7
43 year old woman found to have calcifications on baseline preoperative
mammogram
Stereotactic biopsy found IDC
MRI found 7 suspicious breast masses

Bilateral mastectomy with reconstruction was performed
Points
Mammography may underestimate the extent of disease which is easily
detected on MRI
The patient may be prevented from developing recurrent disease with
preoperative MRI


Boca Radiology Group is pleased to offer state of the art services in breast MRI. We use a dedicated high signal to noise breast coil on our 1.5 Tesla magnets. Our protocol combines high bilateral spatial resolution (3D gradient echo with 512 matrix and 2mm slices of both breasts) with multiple acquisition time points to evaluate the kinetics of tissue enhancement following dynamic bolus gadolinium administration. Pathologic tissues can be identified by their morphology (shape and solid/cystic nature) as well as by their vascularity and permeability (kinetics). Special post processing software provided by our partner in breast MRI research, Mevis Technologies has been moved to a more user friendly Windows 2000 Professional interface (DynaCAD™) from the Silicon Graphics platform. This allows rapid evaluation of large breast MRI data sets in 1- 2 minutes with full 4-Dimensional display (3 orthogonal spatial plus time dimensions with color encoding of enhancement curves) as well as automated 3D motion correction (DYNA Motion) and 3D MIP color overlay (Dyna MIP).
We have conducted a prospective clinical trial of breast MRI's ability to stage breast cancer in collaboration with the Weizmann Institute in Israel and Mevis in Bremen, Germany. We have found that MRI of the breast allows more accurate staging of the extent of breast cancer than mammography and ultrasound. Our post-processing techniques yield higher sensitivity and specificity than interpretation of the raw image data alone. Patient management is significantly changed in many cases. For example, detection of more extensive disease in the breast of concern often leads to mastectomy rather than lumpectomy and cancerous lesions in the opposite breast are often discovered.
We are also evaluating newer software applications including 3D motion correction (DYNA Motion), 3D MIP color overlay (Dyna MIP) with our partner Mevis Technologies.
<click here to download a 3 minute video (24MB, wmv format) demonstrating MRI-guided breast biopsy>
Clinical cases:
Case 1
This 61 year old female presented with a dominant mass in the right breast with several other indeterminate lesions seen on mammography.
Mammography
CC view ![]() demonstrates
three masses in the right breast, one behind the nipple and two others
in its medial portion.
demonstrates
three masses in the right breast, one behind the nipple and two others
in its medial portion.
MRI
magnification maximum intensity projection (MIP) view![]() of
right breast demonstrates the same three masses with tumor bridging
between them and extending toward the chest wall.
of
right breast demonstrates the same three masses with tumor bridging
between them and extending toward the chest wall.
MRI
T2 axial slice![]() indicates
cystic nature of subareolar mass.
indicates
cystic nature of subareolar mass.
MRI
subtraction![]() and color
images
and color
images![]() show
rim enhancement around cystic mass.
show
rim enhancement around cystic mass.
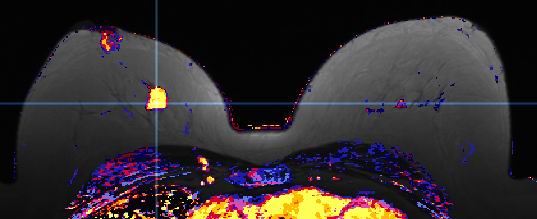
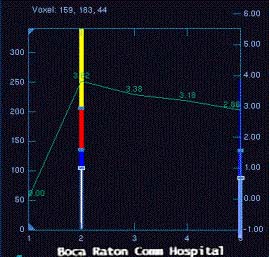
MRI image of color
map of enhancement curves![]() (kinetics
of breast tissue) show intense early enhancement and rapid signal
loss from the dominant mass (typical malignant characteristics).
(kinetics
of breast tissue) show intense early enhancement and rapid signal
loss from the dominant mass (typical malignant characteristics).
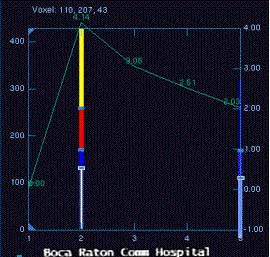
Enhancement
curve from dominant mass![]() .
.
Final Pathology at mastectomy confirmed that the dominant mass represented infiltrating carcinoma with extension of intraductal carcinoma. The subareolar cystic mass represented encysted papillary carcinoma.
Case 2
This second 61 year old female presented with micorcalcifications on mammography.
Mammography
CC view![]() demonstrates
a circled suspicious area of microcalcifications in the left breast
which are better demonstrated on the magnification
view
demonstrates
a circled suspicious area of microcalcifications in the left breast
which are better demonstrated on the magnification
view![]() .
.
Post-processed
color parametric map image![]() demonstrates
a large area of malignant enhancement in the central left breast.
demonstrates
a large area of malignant enhancement in the central left breast.
These findings indicated a much more extensive area of malignancy to the breast surgeon which allowed accurate pre-operative needle localization and subsequent segmental resection with negative margins. Image guided biopsy and surgical pathology specimen revealed extensive intraductal carcinoma (comedo, solid, and cribiform types) with extensive cancerization of lobules. Two small foci of well differentiated infiltrating ductal carcinoma were also identified.
Case 3
This patient
underwent mastectomy, radiation therapy, and subsequent breast reconstruction.
On a follow up clinical examination, there was palpable thickening
raising the question of recurrent cancer. An MRI excluded recurrence. The maximum
intensity projection![]() image
demonstrates enhancing vessels while the color
map image
image
demonstrates enhancing vessels while the color
map image![]() demonstrates
normal arterial vascularity at the margins of the reconstruction.
demonstrates
normal arterial vascularity at the margins of the reconstruction.
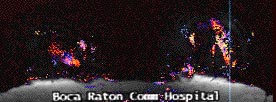
Case 4
An example of
an obvious cancer
in the right breast![]() with
motion artifact resulting in a false eccentric malignant rim of enhancement.
with
motion artifact resulting in a false eccentric malignant rim of enhancement.
The movie![]() demonstrates
a comparison of the original post-processed data set (left hand
images) using a rainbow color map with the most malignant enhancement
demonstrated in red. The motion corrected data set is on the
right. Note that the artifactual background areas of color have
largely disappeared and that the tumor now shows symmetrical peripheral
malignant enhancement.
demonstrates
a comparison of the original post-processed data set (left hand
images) using a rainbow color map with the most malignant enhancement
demonstrated in red. The motion corrected data set is on the
right. Note that the artifactual background areas of color have
largely disappeared and that the tumor now shows symmetrical peripheral
malignant enhancement.
Case 5
58 year old woman with indeterminant calcifications central right
breast. Fatty
Enbloc procedure: DCIS
|
|
|
|
MRI: biopsy cavity with 2cm enhancement posteriorly suspicious for
invasive disease
Surgery: IDC, negative sentinel nodes
Points
MRI can better predict the extent of disease than mammography even
in the fatty breast
Surgical management may change as a result of pre-operative MRI: sentinel
node was performed preventing second surgery, wide localization performed
appropriately to avoid positive margins
Case 6
The patient is a 69 year old woman presenting with a 2 cm left axillary
mass found to be adenoCA compatible with breast primary. Negative prior
mammogram
MRI identified 2 small suspicious masses in the UOQ
|
|
|
|
Diagnostic mammogram & US demonstrated 2 spiculated solid masses
which corresponded
US core biopsy found 2 IDLC
Lumpectomy and axillary dissection was performed
Points
MRI is valuable in the evaluation of a patient with axillary disease
with unknown breast primary
Targeted mammography and US performed after MRI will often identify
abnormalities which then can be biopsied with US or stereotactic guidance
Case 7
43 year old woman found to have calcifications on baseline preoperative
mammogram
Stereotactic biopsy found IDC
MRI found 7 suspicious breast masses
|
|
|
Bilateral mastectomy with reconstruction was performed
Points
Mammography may underestimate the extent of disease which is easily
detected on MRI
The patient may be prevented from developing recurrent disease with
preoperative MRI
|
|