

GUIDE TO MR IMAGING OF THE FOOT &
ANKLE
SNeedell@bocaradiology.com
www.bocaradiology.com
For purposes of MR imaging, the foot is divided into two exams:
1. Ankle/Hindfoot/Midfoot (everything behind metatarsals)
2. Forefoot (metatarsals & toes)
MRIs for tendons & ligaments use "Ankle" protocol unless AOI is specifically in the forefoot.
"Foot" MRIs should be treated as Ankle/Hindfoot/Midfoot MRIs until proven otherwise.
Exceptions: For neuroma, mass, stress fracture,
or osteomyelitis in the forefoot- do a dedicated forefoot (metatarsals
and toes) exam.
• Plantar fibroma & LisFranc fractures- use forefoot protocol but center
over area of interest in the midfoot.
-only image one foot at a time
ANKLE/HINDFOOT/MIDFOOT PROTOCOL
Sagittal T1 & STIR
Axial PD & fat sat T2 (or T2 without fat sat if low field)
Coronal PD
-Ankle tendons and ligaments are best imaged with the foot plantar flexed 15-30°. So avoid using the chimney in a coil. Position the calcaneus in the middle of the coil and the relaxed foot will fit comfortably in the coil at the correct degree of plantar flexion.
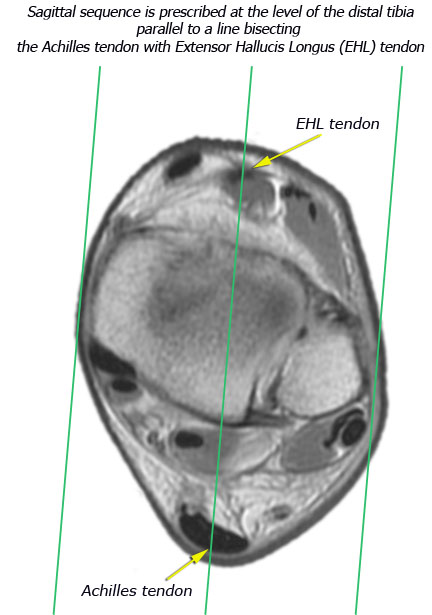
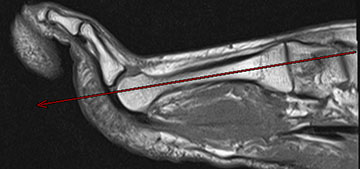
- Sagittal sequence is prescribed off an axial scout at the level of the distal tibia (see figure below) parallel to a line bisecting the Achilles tendon with the Extensor Hallucis Longus (EHL) tendon:
-Inferiorly, axial sections through the ankle should include the fifth metatarsal base.
-Superiorly, axial images should include about 3 cm above the level of the ankle joint. If the exam is specifically to evaluate the Achilles tendon, make sure sagittal and axial images include the Achilles myotendinous junction.
-Axial images can be angled slightly with the tibiotalar joint, but it's better to do straight axials than to oblique too much (see figure below).
FOREFOOT MRI
FOREFOOT MRI

|

|
|
(long axis) |
|
- Place patient prone to image forefoot whenever possible, especially when evaluating for Morton's neuroma.
- Look at the sagittal or longitudinal STIR images before you prescribe the transverse sections so that you can be sure you've covered all the pathology (bright signal on STIR = edema = pathology).
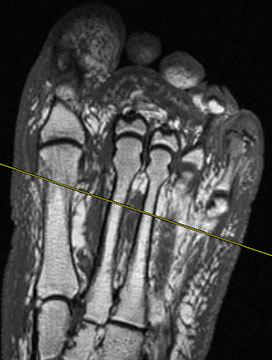
- Forefoot images should be prescribed off a short axis scout at the level of the MTP joints.
 |
 |
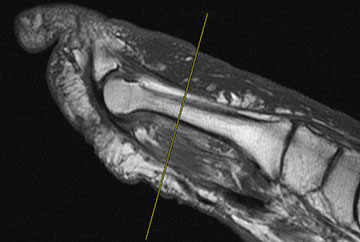
| Long axis bisects the 2nd/3rd metatarsal heads at level of MTP joints on a short axis scout (left image) and parallels the 2nd/3rd metatarsal shafts on a sagittal scout (right image) | |
 |
 |
Prescribe sagittal plane perpendicular to longitudinal Rx at level of MTP joints (left image) and parallel to the 2nd/3rd metatarsal shafts (right image) |
|
 |
 |
| Short axis (transverse) views are perscribed perpendicular to the 2nd/3rd metatarsal shafts | |
- Always mark region of concern with a Vitamin E or fish oil tablet.
- Use small FOVs
Longitudinal T1 (1mm) & STIR (3/0.5mm)
Transverse T1 & STIR (4/1 mm)
Sagittal PD (or T1 if to evaluate infection) & STIR (4/1 mm)
If the patient has had prior neuroma surgery then add a transverse post gad T1W (with fat sat if available)
Plantar fibroma & LisFranc fractures of midfoot
If the area of concern is isolated to the midfoot, such as plantar fibroma, then center the coil over the area of interest & use forefoot protocol.
MATRIX:
If you have enough signal, use 512 x 256 for T1W sequences. STIR & T2 fat sat can be 256x192.