

Cardiac Imaging Services
Department of Radiology
Boca Raton Regional Hospital
RAYUS Radiology, Florida Southeast
 |
 |
 |
 |
Click on icons to navigate to separate discussion pages including images and movies
Background
Cardiovascular disease (CVD), including heart disease and stroke, remains the leading cause of death in the United States despite improvements in prevention, detection, and treatment. CVD is no longer thought of as a disease that primarily affects men as they age. It is a killer of people in the prime of life, with more than half of all deaths occurring among women. Coronary artery disease affects more than 70 million Americans (one quarter of our population) with close to one million deaths per year in the United States. Over 6 million hospitalizations each year are due to cardiovascular disease. For every person who dies from a heart attack or angina, 18 people live with these conditions. For every person who dies from a stroke, seven people cope with the consequences of a non-fatal event. Many of these survivors are disabled and cannot lead productive lives. They also are at high risk for additional events. These numbers are increasing as the epidemic of heart disease and stroke continues.
The economic impact of cardiovascular disease on the U.S. health care system continues to grow as the population ages. The cost of heart disease and stroke in the United States is projected to be $394 billion in 2005, including health care expenditures and lost productivity from death and disability.
Risk factors include advanced age, family history/genetic susceptibility, obesity, smoking, altered lipid metabolism including elevated LDL cholesterol and fatty acids in the blood, chronic diseases such as diabetes, high blood pressure and kidney failure. Current preventative measures include improved diet and nutritional status, exercise, smoking cessation, stress reduction, and medications such as statins, aspirin, and anti-hypertensive agents.
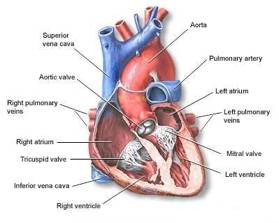
Anatomy
 |
 |
Schematic of cardiac and adjacent
structures viewed
from the patient’s front. |
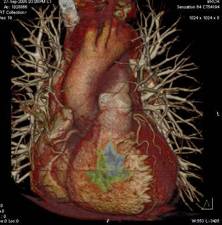
Volume rendered post processed image of the heart
from a 64 slice CT data set.
|
Standard Cardiac Imaging Tests
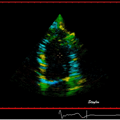
Echocardiography
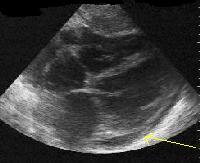
This procedure uses non-invasive ultrasound to image the moving heart either through the chest wall or more invasively (under anesthesia or strong sedation) by passing an ultrasound transducer through the esophagus (food pipe) behind the heart to get closer and more detailed views of the heart which cannot be obtained using the more conventional method. This technology is relatively cheap and widely available. It is however, highly dependent on the operator of the equipment, type of equipment, and level of skill of the interpreting physician.
Echocardiography can be very useful in the acute setting such as in the emergency department and hospital as well as in outpatient settings such as a cardiologist’s office. It is particularly useful in assessing heart muscle and valve function. It can also detect abnormalities of structures near the heart such as the pericardium, aorta, etc. More advanced software packages allow better quantification and visualization of abnormalities. When combined with pharmacological stress testing, it is possible to detect coronary artery blockages by noting wall motion abnormalities when the heart muscle is stressed. This modality cannot reliably visualize the coronary arteries except in very small children.
 |
 |
4-chamber view obtained through the
chest wall, which shows a small pericardial
effusion (fluid collection around the
heart)
|
Mitral Valve
prolapse – dysfunctional
mitral valve which protrudes backwards
into the left atrial chamber of the heart.
|
Nuclear medicine stress testing
This test was first established using two dimensional acquisition techniques in the 1970’s and during the 1980’s three dimensional imaging (SPECT) became the standard. Radioactive pharmaceuticals are injected into the patient while the patient is at rest and also while the patient’s heart is stressed either with exercise or with drugs, which speed up the heart or dilate the coronary arteries. The most common radio-pharmaceuticals for imaging in use are Thallium 201 or Technetium Sestamibi. Either or both may be used for imaging in a comprehensive examination. The heart may be stressed with interventions including treadmill exercise, Dobutamine, or Adensoine administered intravenously.
After the patient is injected, a nuclear medicine camera detects the emitted radiation from the patient and images are reconstructed by a computer which reflect the relative blood flow in the heart both at rest and when stressed. Significant coronary artery blockages (generally greater than 70% of the diameter of the vessel) usually result in relative perfusion (blood flow) to that segment of the heart as being displayed as less than normally perfused heart tissue on these kinds of images. If both the resting and stress images show defects, the tissue will be assumed to be dead (the patient has experienced a heart attack in the past).
There is an abundance of scientific literature that stress testing can non-invasively detect severe coronary artery blockages and can offer prognostic information (predict future heart attacks). It however suffers from several disadvantages;
- It involves radiation – total whole body dosage can range from 10 to as high as 27 mSv (milisievert) for thallium studies. For sake of comparison, the natural background radiation gives the average person an effective dose rate of around 3.5 mSv/year.
- The test is time consuming for both the patient and the department. It may take more than 4 hours and need to be performed over two successive days.
- Its sensitivity for detection of coronary artery blockages greater than 70% is only around 70-75%. This means that one in four patients will be falsely told that they do not have any significant coronary artery blockages.
- It cannot detect coronary artery disease at an early stage and cannot reliably exclude coronary artery disease at any stage.
- It commonly misses high-grade lesions in obese people and those who have triple vessel disease (all coronary arteries have significant blockages).
- Low spatial resolution – will routinely miss sub-endocardial ischemia (partial thickness of the heart tissue being under perfused). It will also frequently miss dead heart tissue in patients who have had smaller heart attacks.
- The test will result in false postives (normal patients being told that they may have blockages) which then result in unnecessary anxiety and testing including cardiac catheterization.
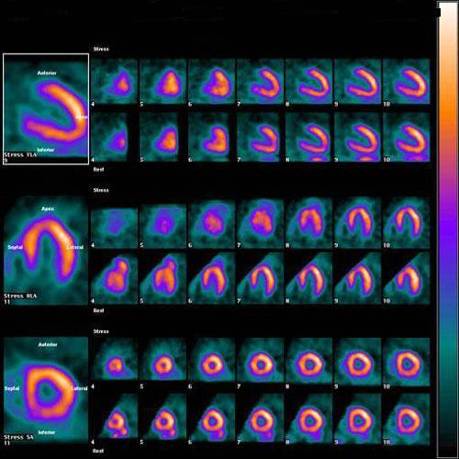 |
| Example of two day Tc-SestaMIBI normal stress and resting SPECT cardiac nuclear medicine study. The images are generally displayed in cross section with the heart sliced in three different projections and the stress images are exactly right above the resting ones. The interpreting physician looks for relative differences in intensity and color of the activity. |
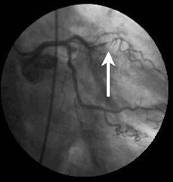
Cardiac catheterization and coronary angiography
More than 4 million patients per year undergo invasive cardiac catheterization each year in the United States with more than 30% of these examinations being normal. Approximately one million undergo revascularization procedures including stenting and coronary artery bypass grafting.
The procedure involves passing a plastic catheter over a guide wire and selectively injecting x-ray contrast into the aorta (main artery coming out of the heart) and the coronary arteries, which supply oxygen to the heart. The major complication rate of this procedure including stroke, heart attack, infection,arterial injury, and death is approximately 1% at most centers. The radiation exposure for diagnostic imaging alone is approximately 3 to 6 mSv but can go above 30 mSv in prolonged interventional procedures. Relatively large doses of iodinated contrast may be used which can be toxic to the kidneys.
Coronary angiography is currently the standard for diagnosing coronary artery disease and is the primary method used to help delineate coronary anatomy. In addition to defining the site, severity, and morphology of lesions, coronary angiography helps provide a qualitative assessment of coronary blood flow and helps identify collateral vessels. Correlation of the coronary angiogram and left ventriculogram findings permits identification of potentially viable areas of the myocardium that may benefit from a revascularization procedure. Left ventricular function can be further evaluated during stress using atrial pacing, dynamic exercise, or pharmacologic agents. Also, valvular function with pressure measurements can be performed to quantify severity of disease.
Limitations of of the diagnostic efficacy of coronary arteriography include:
- The severity of stenosis is generally estimated visually, and estimation is limited by the fact that inter-observer variability may range from 30-60%
- The presence of diffuse disease also may lead to underestimation of stenoses because the narrowed areas are expressed as a percent of luminal diameter compared with adjacent normal coronary segments, and, in diffuse disease, no such segments exist.
- Early coronary artery disease will not be detected unless there is a visible narrowing of the lumen of the vessel on the x-ray images.
- Due to the tortuosity (curving), complex branching and overlapping vessel pattern, and limitations on the angles and views, which can be obtained with a rotating x-ray tube around the patient, blockages may be underestimated or not detected at all.
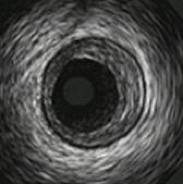
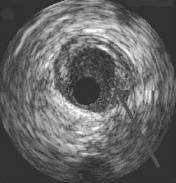
In the last several years, intra-vascular ultrasound (IVUS) has become the gold standard for detection of plaque in the coronary arteries and more precise quantification of blockages as well as plaque characterization. A tiny ultrasound transducer is mounted to a guide wire, which is then selectively placed into each coronary artery. It is technically demanding, needs further standardization, and can significantly lengthen the cardiac catheterization procedure. Therefore, it may not be performed routinely at many centers.
 |
  |
Normal IVUS image |
Extensive soft plaque build up and correlative x-ray angiogram image |