561.391.1728
Osteoporosis is one of the most prevalent diseases of aging women, characterized as a state of heightened skeletal fragility. It is a condition in which the bone mass is too low to resist fracture even with exposure to minimal or modest trauma. The low bone mass per se is not symptomatic; it is the fractures which result that cause signs and symptoms of the disease. Osteoporosis is frequently referred to as the "silent epidemic" as there are no early signs of the disease until fracture occurs.
It is estimated that 15 to 20 million Americans are affected with the disease resulting in 1.3 million fractures per year. The bones most commonly broken are the spine, hip, and wrist. Women at risk for developing the disease include petit women with premature menopause, a family history of the disease, a sedentary lifestyle with inadequate ingestion of calcium, cigarette and alcohol use.
To understand the disease osteoporosis more completely we must understand the normal turnover of bone. Bone is an active living material which Is continually being remodeled. It is broken down in a process called resorption and is rebuilt in a process called formation. These processes occur throughout our life. Until age 35, formation occurs more then resorption, and bones are therefore being built. Our bones reach a peak mass or density at approximately age thirty-five. From that time on resorption occurs more significantly than formation and therefore there is the tendency to lose bone mass as we age.
Estrogen is a hormone which is known to slow down bone loss and promote absorption of calcium from our diet. As women reach menopause, estrogen levels drop significantly as the ovaries decrease their production of the hormone. This results in a dramatic increase in bone loss typically seen around the time of menopause. Approximately 55% of bone loss in women is seen the first 7 years after menopause. The mainstays of prevention of the disease are estrogen replacement therapy and adequate calcium intake.
Now, women with a history of breast cancer may also be at risk to develop osteoporosis particularly if they have an early induced menopause due to chemotherapy. How can we know who is at risk for the disease? How do we diagnose it and how can it be treated if estrogen replacement therapy cannot be given due to the history of breast cancer?
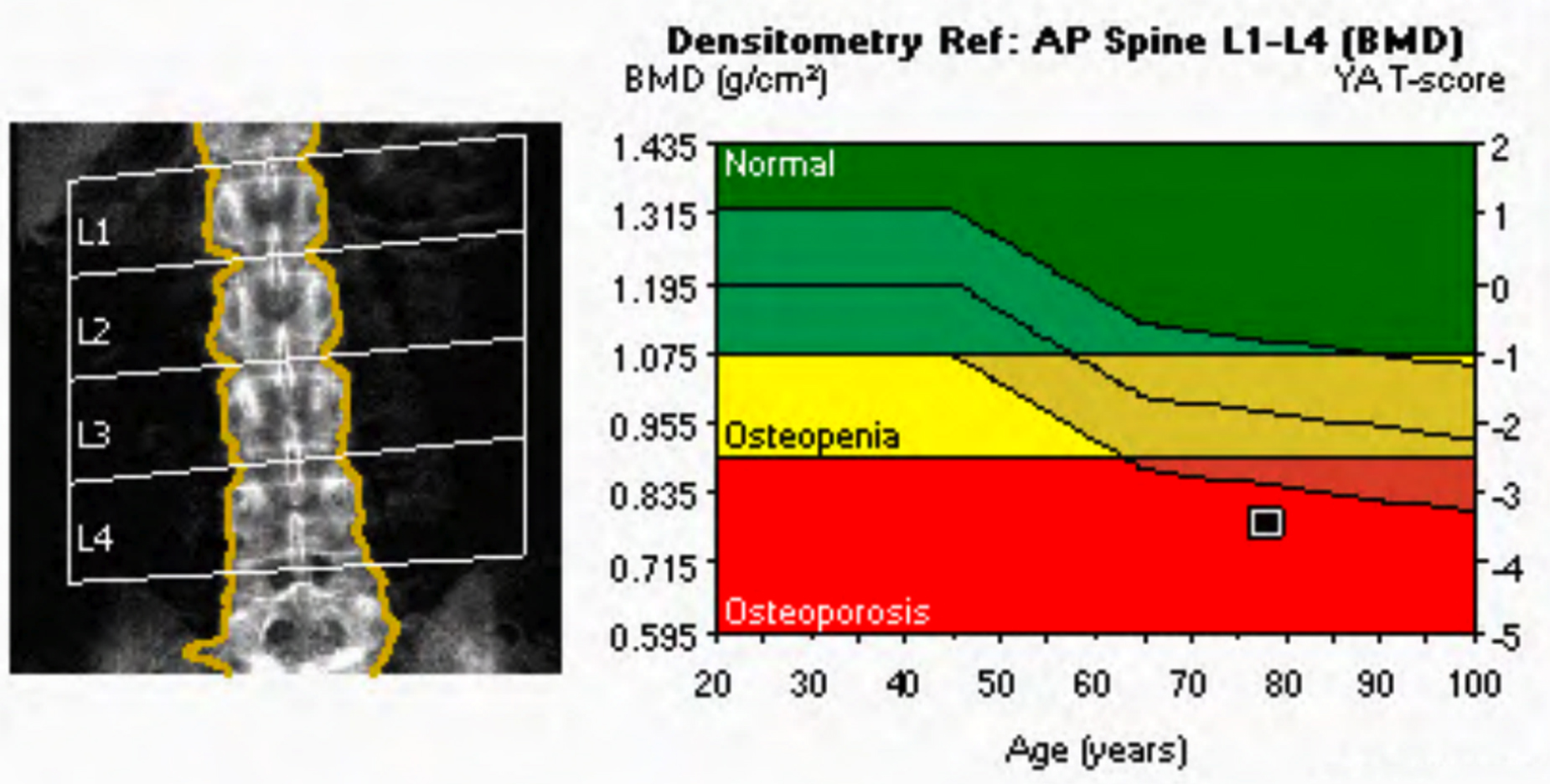
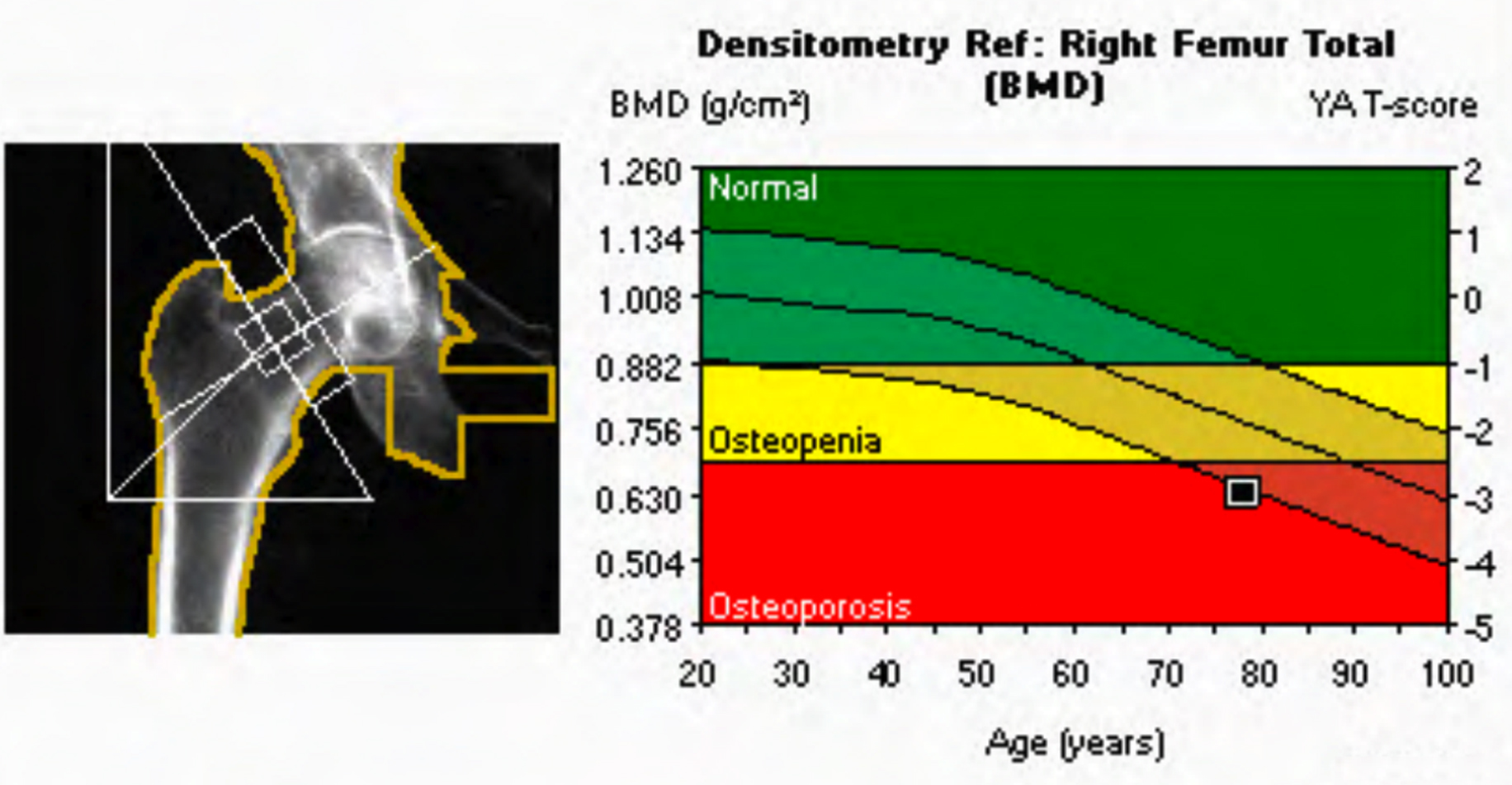
Currently, to diagnose the entity, we are performing bone mineral densitometry on our patients with a baseline exam around the time of menopause. This exam is called dual energy x-ray absorptiometry (DEXA) and uses low dose x-ray to determine bone density. The bone density value is then used as a predictor of bone fragility and susceptibility to fracture. If the bone density is found to be normal, monitoring it in several years may be recommended. It is encouraged to maintain a healthy diet and lifestyle, to supplement the diet with 1600 mg. of elemental calcium per day, and continue weight bearing exercises.
If the bone density is low or abnormal, again the initial recommendations would be to supplement the diet with calcium and develop a weight bearing exercise program. These lifestyle changes may prevent further bone loss. If, however, on repeat bone densitometry a progressive decrease in bone density is noted, additional therapy may be recommended. Current therapies including non-hormonal agents such as Fosamax, have been approved by the FDA for the treatment of osteoporosis. Other treatments are also available including calcitonin nasal spray and other biphosphonates.
Currently, there is no cure for osteoporosis, but there are Pharmacological and nonpharmacological measures available to decrease the rate of bone loss and to prevent future fracture. Early detection, again, becomes important because the progression of the process can be slowed down if detected early.
If you would like more information about osteoporosis or bone densitometry, contact your primary care physician or call the Women's Center at BRRH or RAYUS Radiology, Florida Southeast.


ADA Compliance Policy: In accordance with the American with Disabilities Act, Boca Radiology Group strives to ensure that our web site is accessible to individuals with disabilities. If you have any questions or suggestions regarding the accessibility of this site, please contact us via email or call us at 561.391.1728, so we can ensure you receive the information you are seeking.
© 2023 All Rights Reserved